Implementation challenges
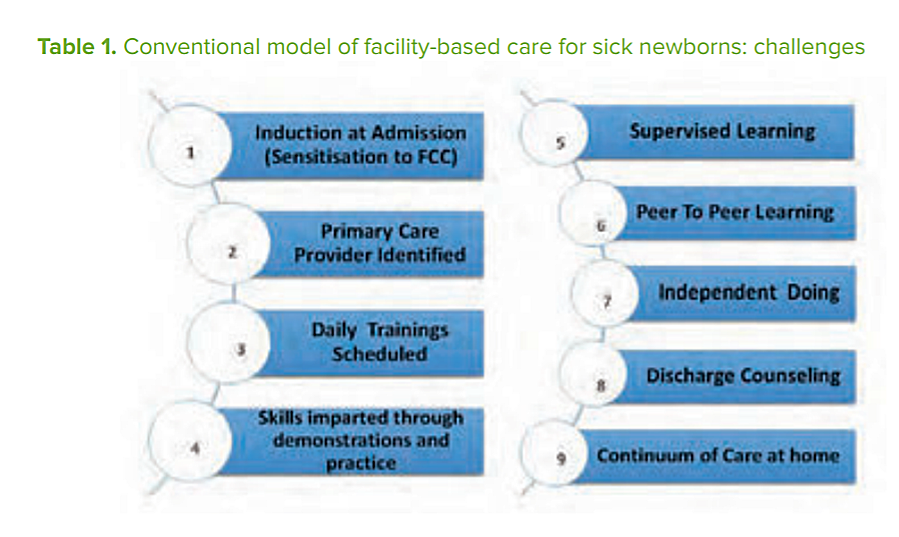
To implement FPC, three important domains need to be addressed: the infrastructure/ design of the unit (physical comfort to families); staff attitudes (empathy and support towards families); and practices that empower family caregiving. Figure 1 sets out the process of operationalizing FPC at a neonatal unit, from admission to discharge and care at home.
The process appears simple but is deceptively challenging to implement, primarily because it is not easy to persuade providers to accept parent-attendants as partners in care. Underlying reasons may include feelings of diminished authority while being watched by an informed parent, and being held to account to deliver a high standard of care.
Providers are also expected to train parents, address their needs for information, guidance and support, monitor them and provide supportive supervision.
Other important elements include effective and respectful communication and carefully planned and executed joint decision-making. Importantly, it must be remembered that the primary responsibility for medical care rests with the provider at all times, and cannot be transferred to the parents. Despite these challenges, once the providers are on board the entire culture of a neonatal intensive care unit changes, quality of care improves and newborns survival rates increase.

Evidence of impact
In externally evaluated qualitative research at Ram Manohar Lohia Hospital in 2016, acceptability of and positive attitudes towards FPC were documented among both health-care providers and families. Additionally, parents continued to use their caregiving skills at home.
The Norway–India Partnership Initiative has revealed the following:
- implementation started in 85 neonatal units in three states with state funding;
- 13,213 (75%) mother and family members received capacity-building FPC sessions;
- 5,548 (86%) newborns below 2,000 grams were provided with kangaroo mother care until discharge;
- initial assessment of mother- y dy s showed rates of exclusive breastfeeding at 86%, and continuation of kangaroo mother care at home at 75%; and
- post-discharge mortality reduced from 7% to 2.7% in the implementing districts.
 Looking forward
Looking forward
Now established as a national programme, FPC led to a paradigm shift in the treatment of sick newborns, covering all components of nurturing care. FPC primarily benefits the poorest and most vulnerable, because they use public sector facilities where staffing ratios are low and quality of care is often poor. It may also improve gender equality by involving both mothers and fathers equally in caring for their newborn children. With the recent release of National Operational Guidelines on Family Participatory Care in 2017 by the Ministry of Health and Family Welfare, states across India have planned and budgeted for scaling up of FPC. In this way FPC will link ECD from the health facility to the community by empowering parents of babies who had the toughest start in life because of being born small or unwell.
Endnotes:
1 Verma A, Maria A, Pandey RM, et al. Family-centered care to complement care of sick newborns: a randomized controlled trial. Indian Pediatr 2017. 54:455–459. http://indianpediatrics.net/june2017/455.pdf (accessed 17 May 2018).
2 For example see: Session 2 – Developmental supportive care https://youtu.be/ALoGXC6-RQk (accessed 17 May 2018).
Acknowledgements: This profile was developed in support of Nurturing Care for Early Childhood Development. A framework for helping children to survive and thrive to transform health and human potential.
Writers: India: Mrs Preeti Sudan, Mr Manoj Jhalani and team, Mrs Vandana Gurnani, Dr Ajay Khera, DR PK Prabhakar, Ministry of Health, Government of India; Prof. Arti Maria and team of Dr RML Hospital, New Delhi, India; Dr Harish Kumar, Dr Ashfaq, Dr Dipti Jhpiego NIPI Team; State Health Societies.
Acknowledging all newborns and their families.
Contributors to development and review: Matthew Frey, Bettina Schwethelm. Design: PATH. For more information, please see www.nurturing-care.org or contact NurturingCare@who.int